- Whitepaper
Clinical supply chain planning

Clinical supply chain planning in life sciences is an increasingly complex process due to regulatory pressures, the time it takes to bring new drugs to markets, and internal dependencies on systems and non-clinical organizational support. At the core of most of these organizations are scientists who have become planners using Microsoft Excel. Data is scattered, vastly different by protocol, and lacking in integration across different sites, or contract manufacturing organizations (CMOs). Because the dosage, formulation, and state are still being finalized as an R&D activity, the data is constantly changing and isn't supported by the MDM governance programs required for ERP systems.
Having planning processes that can run at a program level across multiple trials and understand each trial's contribution to the program is imperative to maximize the understanding of the efficacy and safety of new candidates and optimize the benefits to prospective patients by improving speed to market in a safe, qualified manner. Planning each protocol requires an understanding of:
- The purpose of the trial
- Specific patients' eligibility to join
- How many patients will enrol (timing of enrolment and assumptions around longevity)
- Combinations with other drugs
- Frequency of dispensation
- Dose and form
- Efficacy/safety
The end-to-end planning for a clinical trial program requires companies to develop a target operating model (TOM) or blueprint for how to effectively plan for this inherent complexity given the unknown nature of the supply chain. The core TOM is similar to its commercial counterpart but with some nuanced considerations that alter demand/supply balancing:
- Data management requires the continuous monitoring of ever-changing data. Best practices involve appointing lifecycle managers to facilitate timely and accurate data management
- Demand planning is based on planned enrollment dates with the number of patients, test groups, and sample sizes within each test group
- Supply planning requires estimates of material availability and, for biologics especially, an impact on shared equipment with commercial as well as an integrated plan with CMOs
- Distribution requirement planning requires collaboration with 4PLs over customs/shipping/ logistics concerns be aligned early to prevent changes that may have impacts on the product between the depot to the clinic
These process nuances require specific capabilities that best-in-breed planning systems need to support. Any advanced planning system (APS) should have the following 12 clinical planning capabilities:
- Agile lifecycle management (LCM) processes that include supply chain master data management
- Program review as part of the clinical sales and operations planning (S&OP) process
- Underpin all supply chain nodes in a single environment, even if components of the supply chain are sourced in different instances of the ERP system
- A study design (including double-blinded) that is scalable to meet country-specific approval dates
- Calculated demand curves based on study design
- The ability to update demand and include internal R&D activities in the demand picture
- Incorporate both clinical and commercial nodes of the same supply chain in a unified, transparent fashion
- Manage regulatory approvals by country and balance demand and supply with jurisdictional approvals
- Incorporation of stability protocols in the supply
- The ability to manage comparators effectively
- Manage 3PL and 4PL partners in a way that is commensurate with the relationship
- Customized KPIs and reporting
These key capabilities are outlined across the different stages of the TOM below and highlight best practices to consider when deploying a clinical planning APS tool.
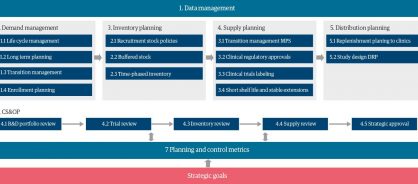
Data management
Data management is a challenging, ongoing process that requires precision over years of changes to the data as a molecule progresses through trial stages. A complete material master data, bill of material (BOM), and network build are crucial for accurate planning.
In early-stage trials, the SKU data and BOM data maturity data are low. Planning is taking place at a high level over a long-term horizon. It is important to identify and maintain the essential attributes to enable top-down independent demand propagation and initial supply response with allocations of capacity. This pro-cess needs to consider the trial timeline and identify when master data requires updates. This will ensure that as a study reaches new phases throughout its lifecycle, data maturity will enable other processes with the right quality all the way through to near-term execution when the data has to be accurate for planning and regulatory reasons.
Demand management
The demand management process is based on planned patients' enrolment or placeholder demand (through planning BOMs) depending on the phase of each study's approval. LCM is the first step in this process. This is an ongoing process with continual iterations that require precision in executing the right changes at the right time. This will ensure that demand calculations can proceed from a long-term strategic plan (ideas not yet approved for studies) to a near term execution window in which studies are ap-proved and have real demand. Following the project initiation until the study is approved internally, demand planning is based on assumptions of the total number of patients to be recruited in a given market. At this stage, long-term planning is typically set up as planning materials at the study level. After internal company approvals, there is a transition to execution SKUs, and the forecast shifts to a clinical trial forecast. After study initiation the forecast will become independent demand with confirmed patient enrolment shared by local entities coordinating that activity. The execution process is then taken over by the ERP system.
Inventory planning
For clinical trials, the service level is always set to 100%, and there is no room for delays or late fulfilment. Inventory planning and time-phased strategic stock levels are key to achieving that service level. The key variable and starting point for inventory-level setup will be planned recruitment completion. Supply managers responsible for setting the right levels will tend to keep higher stock if recruitment is yet to be completed to prevent volatility, enrolment acceleration, or general increases versus planned forecast. Throughout the course of the study (and after the first patient receives the first dose of the product), strategic stock needs to be specified as demand/and supply stabilize and becomes less variable. Using time-phased inventory will support the project ramp-down with last patient/last visit, minimizing inventory that will expire.
Supply planning
The supply planning process has a strong correlation to LCM. Most of the steps within master production scheduling activities, including supply propagation, supply-to-demand allocation, and the firming up of planned orders are equivalent to the commercial drug business processes. Accordingly, supply planning will typically take place on a planning material, including firming of planned orders. This part of the process should be fully handled in APS without interaction with ERP systems. When approval is in place and actual material is created, with the right maturity of master data, firm orders can be transitioned and integrated into the ERP system for execution. Nuances in supply planning processes include:
- Blinding the supply plan where different SKUs in the study are packaged together as to be indistinguishable
- Stability programs where R&D is planning to extend the shelf life at different markers to be able to plan supply from the initial and fast-to-expire products to a more stable supply plan with less impactful expiry
- Accelerated release where the next level of the BOM may be completed prior to when the long lead time testing results are achieved
Distribution planning
The key focus of distribution planning is to make sure that products reach the clinical sites where actual dispensation to patients is taking place, on time. Firming of distribution orders is equivalent to firming MPS for make/buy items, where availability of the supply needs to match the demand due date. To mitigate the risk, in-transit stock should be added to inventory and considered in the netting of available supply. While building a distribution plan, the study design must be considered to buffer risks in the execution phase through strategic and/or cycle stock.
Clinical S&OP
The clinical S&OP process in R&D departments is the same as commercial drug production, with a monthly cadence. In commercial pharmaceuticals, the S&OP process is typically at the brand level, whereas in clinical S&OP, the review takes place at the program or even study level. The clinical workflow typically has five steps:
- Program review
- Demand review (trial review)
- Inventory review
- Supply review
- Approval (single approval for clinical)
Planning and control metrics
Planning and control metrics support the current-state assessment of day-to-day work as well as decisions across the whole clinical S&OP process. APS tools can customize dashboards and scorecards to meet the clinical business across a range of KPIs. These typically include:
- Regulatory date changes by country
- On-time, in-full to net requirements (demand)
- Strategic stock attainment
- Expiry risk
- Capacity utilization
All of these unique nuances in clinical supply chain planning mean no out-of-the box APS exists to meet clinical trial requirements. To overcome this, life science organizations are increasingly partnering with service providers to design a digital clinical trial solution that works with existing APS tools.
Download the full whitepaper for a detailed analysis of the APS capabilities required for clinical supply chain planning


Share